Quality improvement can largely be defined as the ability to collect data to measure the outcomes of current or developing processes and using that data to improve systems of care (Weston & Roberts, 2013). With the ever changing technology and health care needs of today’s population, there has been an increased need to better address patient care outcomes and quality of care provided across the continuum. Although quality improvement efforts have been widely accepted in the health care field as a whole, the Institute of Medicine has not only identified the need for improving health care systems, but the need for nurses to act as contributory members of quality improvement teams (IOM, 2010). With that being said, there is a strong link between nursing education and the ability to provide safe patient care. Currently, nurse educators are being challenged to re-design nursing curricula in order to prepare new graduates to contribute to a safe and quality patient care environment (Pauly-O’Neil & Cooper, 2013). It has been identified that nurses are often able to recognize inadequacies in safe, quality patient care but lack the cognitive tools and knowledge necessary to initiate effective quality improvement projects (Kovner, Brewer, Yingrengreung & Fairchild, 2010). To combat this, the Quality and Safety Education for Nurses (QSEN) competencies were developed for inclusion in nursing education to facilitate the development of nurses in regards to providing safe, quality care. QSEN competencies assist to ensure that nurses have the necessary knowledge, skills and attitudes to continuously improve healthcare systems within their clinical arena (Dolansky & Moore, 2013). Including QSEN competencies such as quality improvement in nursing education will allow students to build a toolbox in which they can use in the future to help lead change initiatives for improving healthcare systems and patient outcomes (Murray, Douglas, Girdley & Jarzemsky, 2010).
Nurses are constantly challenged to identify practice gaps between current and best practices. Nurse educators are being challenged to fill the gaps that exist between nursing education and the real-world. The literature shows that current nursing curriculum primarily teaches the students to provide task-oriented care at the individual patient level (Dolansky & Moore, 2013). Dolansky & Moore (2013) would argue that it is imperative to incorporate systems thinking into nursing education. Systems thinking will enhance the learner’s awareness of the interdependencies that exist in people, processes, and services in order to view problems as a whole rather than as a piece (Dolansky & Moore, 2013). One prime example of how nurse educators can incorporate systems thinking is by bridging the educational gap between class room and clinical settings.
Pre-licensure students are often taught theoretical knowledge in class as to how quality improvement affects patient care (Pauly-O’Neil & Cooper, 2013). In most cases, education about quality improvement ends here. The concern is that a connection is not made between the classrooms and clinical. In one study, “data mining” was used to allow students to connect theoretical knowledge gained in the classroom with the ability to collect unit-level data at a clinical site and compare their findings to benchmarks (Pauly-O’Neil & Cooper, 2013). Another strategy was to have students complete near-miss error reports during their clinical rotations (Pauly-O’Neil, 2013). A third strategy to bridge the gap between classroom and clinical is to have students review institutional policy and procedure then partake in a “work-around” activity to observe nursing staff as they perform nursing action (Pauly-O’Neil & Cooper, 2013). This will allow students to begin to develop a watchful eye for areas that are in need of quality improvement.
By integrating quality improvement competencies into nursing education, and bridging the gap between the classroom and clinical arena, this will better prepare nurses to take action to improve patient care when they enter the workforce. Below are a few teaching strategies that were developed to incorporate quality improvement education into a four-year baccalaureate nursing program. The strategies were developed keeping in mind the need for not only incorporating quality improvement into the nursing curriculum, but bridging the gap between knowledge gained in the classroom and the student’s clinical experience.
Dolansky, M. A & Moore, S. M. (2013) Quality and safety education for nurses (QSEN): The key is systems thinking. The Online Journal of Issues in Nursing, (18)3.
Herrman, J. W. (2016). Creative teaching strategies for the nurse educator (2nd ed). Philadelphia, PA: F. A. Davis Company.
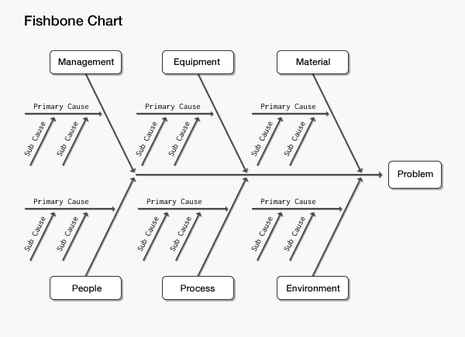
How to use the fishbone tool for root cause analysis. (n.d.). Retrieved on 3/18/2017 from https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/FishboneRevised.pdf
Kovner, C. T., Brewer, C. S., Yingrengreung, S., & Fairchild, S. (2010). New nurses’ views of quality improvement education. The Joint Commission Journal on Quality and Patient Safety,36 (1), 29-35.
Murray, M., Douglas, S., Girdley, D., & Jarzemsky, P. (2010). Teaching quality improvement. The QSEN Learning Collaborative. Nursing Outlook, 57(6), 304-312.
Pauly-O’Neil S. & Cooper, E. E. (2013). Addressing gaps in quality and safety education during pre-licensure clinical rotations. Nursing and Health Professions Faculty Research and Publications, (11)3, 65-70. Doi: 10.5430/jnep.v3n11p65 Weston, M. & Roberts, D. W. (2013). The influence of quality improvement efforts on patient outcomes and nursing work: A perspective from chief nursing officer at three large health systems. The Online Journal of Issues in Nursing, (18)3.